Note this article was originally published on apptheneum on July 15, 2014.
Type I diabetes also known as juvenile diabetes is an autoimmune disease primarily mediated by T-cells (a type of white blood cell) that results in the destruction of pancreatic β-cells which produce the body’s insulin hormone. Insulin induces the uptake of glucose by adipose tissue (fat cells) and skeletal muscle. Lack of insulin results in hyperglycaemia (higher than expected blood glucose). The three major symptoms of hyperglycaemia are frequent acute, hunger and thirst, and increased volume of urination. If untreated coma and heart attack can result. Standard treatment is daily insulin injection. This does not perfectly regulate blood glucose levels and over time people with type I diabetes can develop problems with their feet associated with reduced circulation and nerve damage. Cardiovascular disease, retinopathy (eye damage), general nerve damage, kidney disease, and sexual dysfunction are also major problems. The next generation of gene and cell therapies aim to restore glucose sensitive insulin secretion in type I diabetics and thus eliminate long-term complications.
Cell therapy offers much promise but has yet to prove it can overcome certain obstacles. It is based on replacing the destroyed β-cells with either mature donor cells or (theoretically) autologous cells generated from the patient. Unfortunately the underlying disorder reamains and the cells will eventually be destroyed by the immune system once more even with the administration of immunosuppressive agents. This approach also suffers from lack of donors. None the less the initial transplantation method has been proven effective. Human Embryonic stem cells (from donors not the patient) have been used to generate insulin secreting β-like cells. However immunosupression is still required to administer these cells and they suffer from the same long term degradation as donor islets.
Patient derived cells are potentially a better option as they do not require a donor and would not trigger an anti-self immune response when reintroduced to the patient. Type I diabetes patient derived induced pluripotent stem cells (iPS) have been generated from skin biopsy fibroblasts and insulin-producing and glucose-responsive β-like cells have been differentiated from these cells. Minicircle DNA vectors for eukaryotic cell transfection lack any bacterial or viral sequence. In contrast to standard vectors that contain bacterial sequences transgene expression from minicircle vectors can be sustained for weeks. They also have the advantage that they do not integrate into the host cell genome which eliminates concerns of tumourigenic insertion events. Minicircle vectors have been used to generate iPS cells. This provides a basis for the development of treatments for type I diabetic patients based on transplantation of β-like cells differentiated from these minicircle generated iPS.

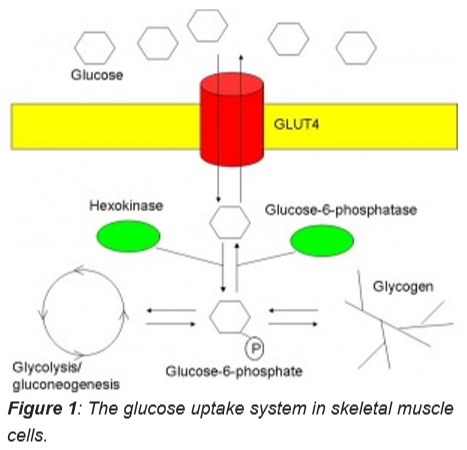
Gene therapy offers a potentially less complicated method of restoring glucose regulated insulin secretion to type I diabetic patients. Furthermore this approach has proven effective long term (reversal of diabetes for greater than 4 years) in a large animal model (induced diabetic Beagle dogs). Callejas et al. targeted skeletal muscle for insulin production. Insulin stimulates both the translocation of GLUT4 to the plasma membrane and the activity of hexokinase (Figure 1). Glucokinase is analogous to hexokinase but is more constitutively active but requires high glucose concentration for maximal activity. In the Callejas et al. study both insulin and glucokinase driven by constitutive promoters was delivered to the dog’s muscle by injection of adeno-associated viral vectors. In these animal hyperglycemia was eliminated and remained so for greater than four years (until the end of the study). There was no evidence of diabetic complications in these animals. The authors aim to replicate these results in pet dogs and eventually human clinical trials. If successful type I diabetes could be treated with a one time procedure that would afford long term protection from diabetic complications.
The liver is an attractive target for type I diabetes gene therapy due to its relative ease of targeting with non-viral vectors in animal models (hydrodynamic injection) and the fact that hepatocytes (liver cells) have an active protein synthesis and constitutive protein secretory mechanism, as well as the ability to sense and metabolically respond to changes in ambient glucose levels. In a recent study minicircle DNA containing modified insulin gene to facilitate liver processing under the control of glucose response elements was administered to chemically induced diabetic rats via hydrodynamic injection. Hyperglycaemia was eliminated for a month following the initial hydrodynamic procedure. This approach is attractive as it is potentially very safe with no DNA integration and no bacterial or viral sequences to trigger immune response. However a delivery method based on the mechanism of hydrodynamic injection needs to be developed for application to patients in the clinic.
The endocrine K cells of the gut are an attractive target as they are glucose responsive and secrete the hormone glucose-dependent insulinotropic polypeptide (GIP) in response to glucose in a temporal pattern very similar to insulin. It has been demonstrated that when the GIP promoter is used to drive insulin expression and introduced into the pronuclei of fertilized mouse embryos, the transgenic mice that are generated express insulin from their K cells. Furthermore when the transgenic mice were treated with Streptozotocin a β-cell toxin they did not develop diabetes in contrast to control mice. On the basis of this research the Canadian company enGene are currently developing methods to target human K cells for type I diabetes therapy.
Gastric G cells, exocrine pancreas and L cells have also been targeted. Thus, there are many options awaiting clinical trial. However a major obstacle to all of the approaches mentioned which is often not accounted for in the studies discussed above is the original autoimmune disease of the patient that caused the destruction of the β-cells in the first place. Fortunately progress has been made in understanding the underlying immune response that triggers type I diabetes however much work is needed to determine an approach that would suppress the autoimmune response in diabetic patients. A very interesting observation and one that could be used to protect novel reprogrammed β-cells is that the adenovirus E3 gene cassette can protect β-cells from destruction in a virus induced mouse model of diabetes.
Further clinical trials for type I diabetes are required to determine which of these promising experimental treatments is the best option for this autoimmune disease.
David Orchard-Webb
Bibliography
Alam, T. et al. Correction of diabetic hyperglycemia and amelioration of metabolic anomalies by minicircle DNA mediated glucose-dependent hepatic insulin production. PloS one 8, e67515 (2013).
Auricchio, A. et al. Constitutive and regulated expression of processed insulin following in vivo hepatic gene transfer. Gene therapy 9, 963-971 (2002).
Callejas, D. et al. Treatment of diabetes and long-term survival following insulin and glucokinase gene therapy. Diabetes 62, 1718-1729 (2013).
Chen, Z.-Y., He, C.-Y., Ehrhardt, A. & Kay, M.A. Minicircle DNA vectors devoid of bacterial DNA result in persistent and high-level transgene expression in vivo. Molecular therapy 8, 495-500 (2003).
Cheung, A.T. et al. Glucose-dependent insulin release from genetically engineered K cells. Science 290, 1959-1962 (2000).
Jia, F. et al. A nonviral minicircle vector for deriving human iPS cells. Nature methods 7, 197 (2010).
Maehr, R. et al. Generation of pluripotent stem cells from patients with type 1 diabetes. Proceedings of the National Academy of Sciences 106, 15768-15773 (2009).
E. Tudurí et al. Reprogramming gut and pancreas endocrinecells to treat diabetes. Diabetes, Obesity and Metabolism 13, 53-59 (2011).
Von Herrath, M.G., Efrat, S., Oldstone, M.B. & Horwitz, M.S. Expression of adenoviral E3 transgenes in β-cells prevents autoimmune diabetes. Proceedings of the National Academy of Sciences 94, 9808-9813 (1997).